|
|
International Journal of Arrhythmia 2011;12(2): 50-53.
|
Case
A 23-year-old man with Wolff-Parkinson-White
syndrome and atrial fibrillation was referred for
catheter ablation. He had recurrent paroxysmal
palpitations since childhood. He underwent direct
current cardioversion of preexcited atrial
fibrillation (AF) 15 months before admission. Past
medical history was unremarkable. Physical
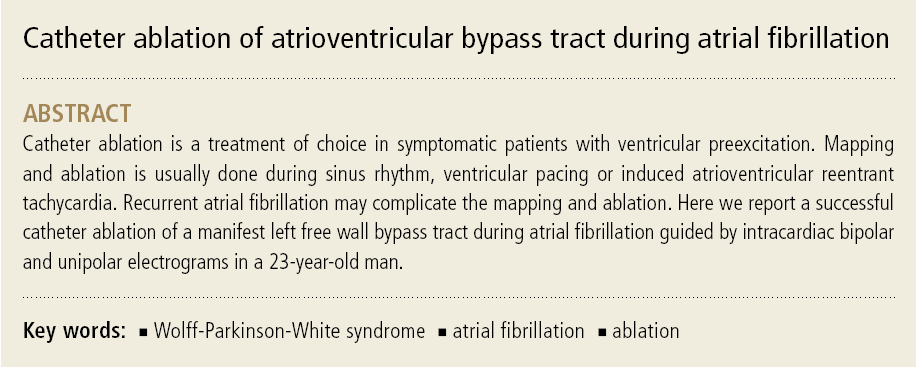
examination was normal. A 12-lead electrocardiogram
shows delta waves with negative
polarity in lead aVL and positive polarity in lead V1,
suggestive of left free wall accessory pathway (Figure 1A). Echocardiography was normal.
After an informed consent was obtained, a
cardiac electrophysiologic study was performed
under fasting conditions. Sedation and analgesia
was administered using propofol and morphine.
Multipolar electrode catheters were advanced into
the femoral veins and positioned in the right
atrium, His-recording region, right ventricular
apex and coronary sinus. Preexcited AF occurred
spontaneously. During preexcited AF, the shortest
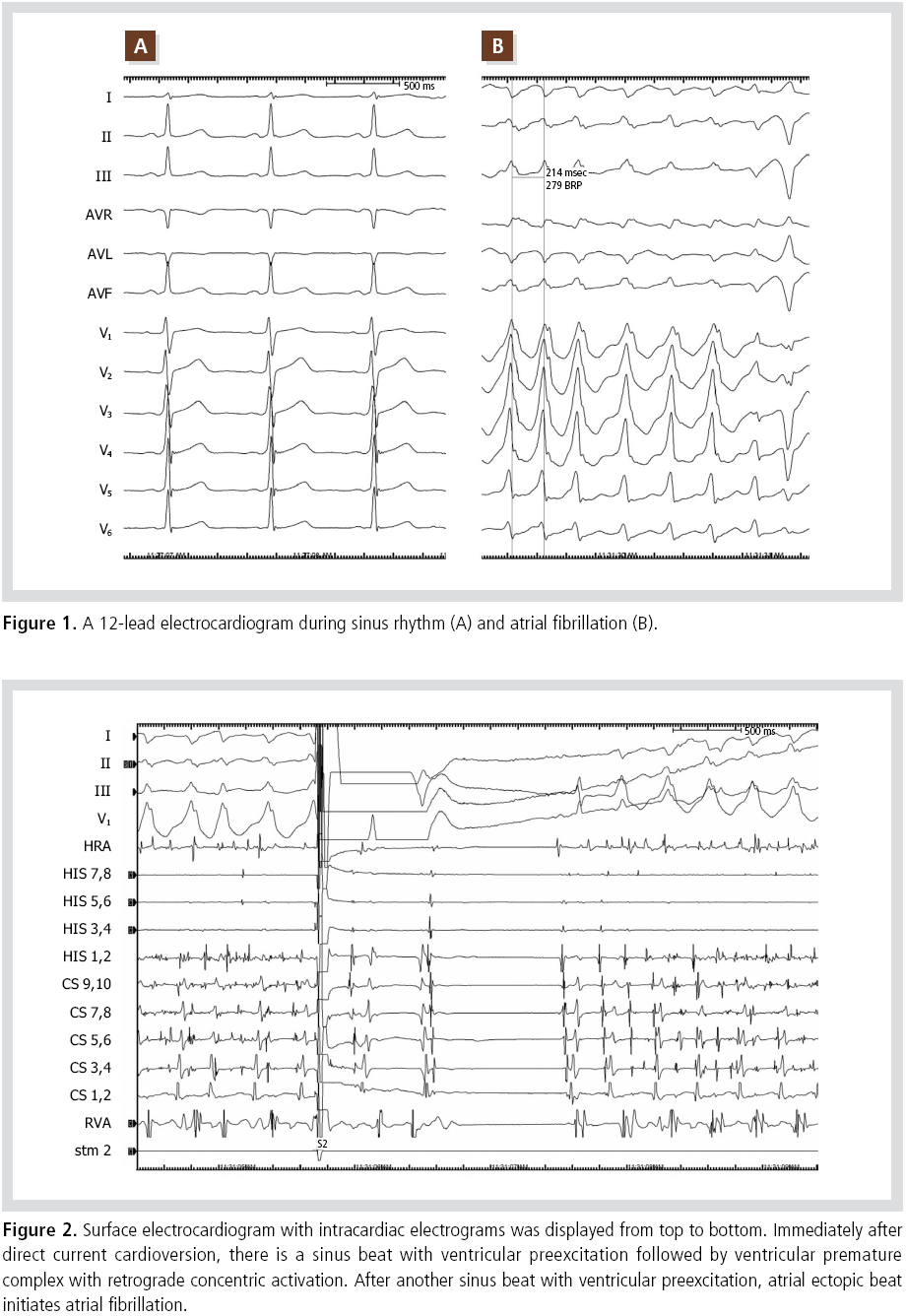
RR interval was 214 ms (Figure 1B). Immediate
recurrence of AF by an earlier atrial ectopy at the
high right atrium was noted after each attempt of 3
successful direct current cardioversion (Figure 2).
Based on the clinical history of preexcited AF, short
RR interval during AF and atrial vulnerability
during the study, catheter ablation of the bypass
tract was performed.
After successful transseptal catheterization and
heparinization (100 units/kg), a 7-Fr conventional
ablation catheter with a 4 mm distal tip was
advanced through the transseptal sheath. Earlier
ventricular activation was noted at the lateral
mitral annulus where ventricular electrograms,
preceding the onset of delta wave by 25 ms, and QS
pattern on unipolar electrograms were noted
(Figure 3A, B). Application of radiofrequency
energy (50 W, 60 °C) at the site abolished the
ventricular preexcitation in 4 seconds (Figure 3C).
Total energy delivery time was 140 seconds.
After restoration of sinus rhythm by an electrical
shock, there was no antegrade and retrograde
conduction via the bypass tract. There was only
retrograde nodal conduction without antegrade
dual AV node physiology. AF was induced by a
single atrial extrastimulation (A1A1 500 ms, A1A2
220 ms) and was electrically cardioverted to sinus rhythm. During infusion of isoproterenol up to 20
mcg/min, there was no atrial ectopic beat or AF.
Procedure was finished without complication. Total
procedural time, fluoroscopic time was 80 and 6
minutes, respectively.
He had no recurrence of ventricular preexcitation
or AF during 1- year-follow-up period.

Discussion
We report a successful catheter ablation of
antegrade accessory pathway during AF guided by
intracardiac electrogram analysis.
Catheter ablation of bypass tracts is established
treatment for symptomatic patients with manifest
or concealed bypass tracts.1 Targeting of the
ablation site is determined by local AV interval,
local V-QRS onset interval during sinus or atrial
pacing or local VA interval during ventricular pacing or VA interval during AV reentrant
tachycardia.2,3
If AF complicates the ablation procedure of
ventricular preexcitation, electrical or pharmacologic
cardioversion can be tried. As in this case electrical
cardioversion requires deep sedation and even
immediate recurrence of AF may complicate the
procedure. Pharmacologic cardioversion can be
tried. However, amiodarone, the only available
intravenous antiarrhythmic drug effective in AF in
Korea is not useful because it has a delayed onset
compared with other class IV drugs and may block
accessory pathway conduction.
Hindricks et al. reported that mapping of a,site
with Kent bundle potential and analysis of unipolar
electrogram recorded at the mapping catheter was
useful in targeting the optimal target sites in
preexcited AF.4 We could not record Kent bundle
potential at the target site. However, a unipolar
electrogram was used for determining the optimal
target site. Multiple AF waves can distort the local
ventricular electrogram and hamper the analysis of
local activation time especially in the distal bipolar
electrogram. Because there was no atrial signal in
the unipolar electrogram, unipolar electrogram can
be invaluable to determination of local activation
time. To obtain noise-less unipolar electrogram, an
independent electrode in the inferior vena cava
should be used as an indifferent electrode rather
than the Wilson central terminal.
Regarding the origin of atrial fibrillation in this
patient, the right superior pulmonary vein or the
superior vena cava is the probable site of origin.
Because ① ablation of the bypass tract is sufficient
in eliminating atrial fibrillation, especially in young
patients with preexcited atrial fibrillation and ②
atrial ectopy was noted only transiently after
electrical cardioversion, mapping and ablation of triggering sites was not attempted.5,6
In conclusion, ablation of the atrioventricular
bypass tract during atrial fibrillation can be
successfully done by analysis of intracardiac bipolar
and unipolar electrogram.
References
- Blomstrom-Lundqvist C, Scheinman MM, Aliot EM, Alpert JS,
Calkins H, Camm AJ,Campbell WB, Haines DE, Kuck KH, Lerman
BB, Miller DD, Shaeffer CW, Stevenson WG,Tomaselli GF, Antman
EM, Smith SC Jr, Alpert JS, Faxon DP, Fuster V, Gibbons RJ,
Gregoratos G, Hiratzka LF, Hunt SA, Jacobs AK, Russell RO Jr,
Priori SG, BlancJJ, Budaj A, Burgos EF, Cowie M, Deckers JW,
Garcia MA, Klein WW, Lekakis J,Lindahl B, Mazzotta G, Morais JC,
Oto A, Smiseth O, Trappe HJ; European Societyof Cardiology
Committee, NASPE-Heart Rhythm Society.ACC/AHA/ESC guidelines
for the management of patients with supraventriculararrhythmias--
executive summary. a report of the American college
ofcardiology/American heart association task force on practice
guidelines and theEuropean society of cardiology committee for
practice guidelines (writingcommittee to develop guidelines for the
management of patients withsupraventricular arrhythmias)
developed in collaboration with NASPE-Heart Rhythm Society.
J Am Coll Cardiol. 2003;42:1493-1531.
- Haissaguerre M, Fischer B, Warin JF, Dartigues JF, Lemetayer P,
Egloff P. Electrogram patterns predictive of successful
radiofrequency catheter ablation of accessory pathways. Pacing
Clin Electrophysiol. 1992;15 (11 Pt 2):2138-2145.
- Grimm W, Miller J, Josephson ME.Successful and unsuccessful
sites of radiofrequency catheter ablation of accessory
atrioventricular connections. Am Heart J. 1994;12:77-87.
- Hindricks G, Kottkamp H, Chen X, Willems S, Haverkamp W,
Shenasa M, Breithardt G, Borggrefe M. Localization and
radiofrequency catheter ablation of left-sidedaccessory pathways
during atrial fibrillation. Feasibility and electrogramcriteria for
identification of appropriate target sites. J Am Coll Cardiol.
1995;25:444-451.
- Haissaguerre M, Fischer B, Labbe T, Lemetayer P, Montserrat P,
d'Ivernois C,Dartigues JF, Warin JF.Frequency of recurrent atrial
fibrillation after catheter ablation of overtaccessory pathways.
Am J Cardiol. 1992;69:493-497.
- Brembilla-Perrot B, Popescu I, Huttin O, Zinzius PY, Muresan L,
Jarmouni S, Nossier I, Schwartz J, Sellal JM, Beurrier D,
Andronache M, de Chillou C, Selton O, Louis P, Terrier de la
Chaise A. Risk of atrial fibrillation according to the initial
presentation of apreexcitation syndrome. Int J Cardiol. 2011 Jan
14. [Epub ahead of print]
|
|
|
|












