International Journal of Arrhythmia 2013;14(1): 28-32.
Untitled Document
ECG & EP CASES
Successful Radiofrequency Catheter Ablation of Scar-related Atypical Right Atrial Tachycardia with Paroxysmal Atrial Fibrillation by Using a Three-Dimensional Mapping System
Yae-Min Park Young-Hoon Kim
Yae-Min Park, MD, Jong-Il Choi, MD, Hong-Euy Lim, MD, Sang-Weon Park, MD, Young-Hoon Kim, MD, PhD Division of Cardiology, Department of Internal Medicine, Korea University Medical Center, Seoul, Korea
Introduction
Conventional techniques for radiofrequency
catheter ablation provide less data regarding
accurate spatial location and preclude accurate
electroanatomical mapping of complex cardiac
arrhythmia. Recent advances in electroanatomical mapping offer advantages over conventional
mapping by reconstructing a 3-dimensional image
of the cardiac chamber.
In this report, we describe a case of paroxysmal
atrial tachycardia (AT) in which a 3-dimensional
mapping system facilitated successful ablation.
Case
A 61-year-old woman presented with recurrent
palpitations. Electrocardiography during the
palpitations showed wide QRS tachycardia (Figure 1),
and 24-h Holter monitoring revealed frequent
unsustained episodes of paroxysmal AT and atrial
fibrillation (AF). She was previously diagnosed with
paroxysmal AF 4 years ago, and it had been wellcontrolled
with antiarrhythmic medication.
However, paroxysmal AT with 1:1 ventricular
conduction frequently occurred and the patient was
highly symptomatic. Therefore, she underwent
radiofrequency catheter ablation for paroxysmal AT
2 years ago. Focal ablation at the high right atrial
septum eliminated AT during the previous ablation
session and she had been stable for 2 years prior to
this event. Echocardiography revealed a mildly
reduced left ventricular ejection fraction (40.5%)
and slightly enlarged cardiac chambers. The
anteroposterior diameter of left atrium was 48.5
mm. Antiarrhythmic drugs were ineffective and
sinus node dysfunction developed. She therefore
decided to undergo catheter ablation for
paroxysmal AT and AF.
An electrophysiologic investigation was performed
by placing a duodecapolar catheter in the coronary
sinus, a decapolar catheter in the high right atrium,
and a quadripolar catheter in the bundle of His.
First, the geometry of the left and right atrium
were obtained using the NavX system (St Jude
Medical Inc., St Paul, MN, USA). We eliminated 4
pulmonary vein potentials by circumferential antral
ablation. Voltage mapping was performed in both
atria; the area characterized by voltages of <0.1
mV was defined as a scar. An extensive area in
right atrium, specifically the high and low crista
terminalis, and the high right atrial septum were
identified as scar zones (Figure 2). We then
attempted to induce tachycardia by rapid atrial
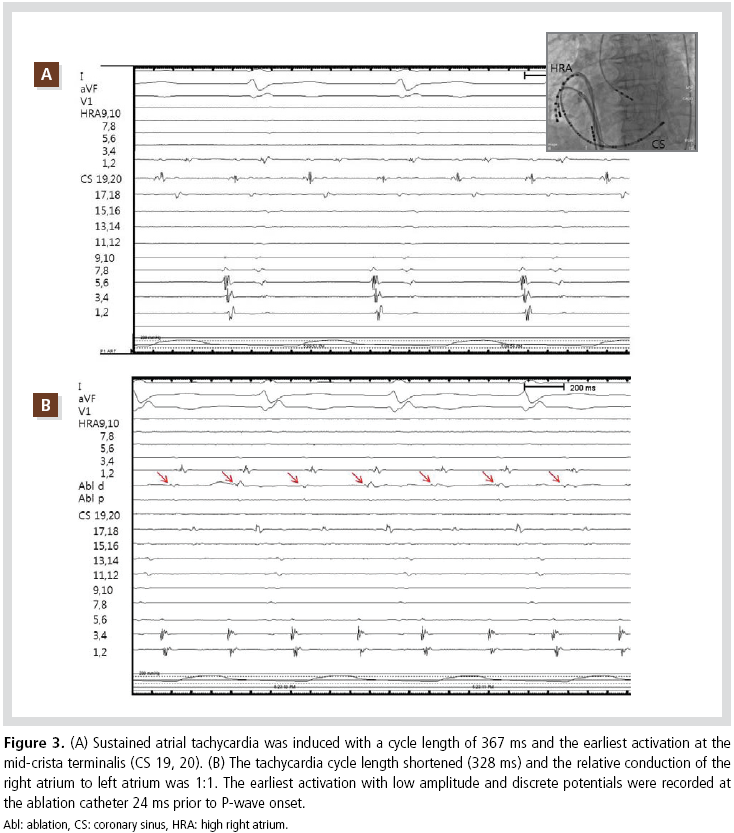
pacing. Sustained AT was induced with a cycle
length of 367 ms. The earliest activation was
observed at the mid-crista terminalis area (CS 19,
20), and the relative conduction of the right atrium
to the left atrium was 2:1 (Figure 3A). The
tachycardia cycle length shortened (328 ms) and
the relative conduction of the right atrium to the
left atrium became 1:1 (Figure 3B). In an electrophysiologic
investigation, entrainment mapping
excluded the cavotricuspid isthmus and left atrium
as part of the tachycardia circuit. Additionally, an
activation map in the right atrium was created. It
revealed slow conduction at the crista terminalis
surrounded by a low-voltage scar zone that spread
centrifugally throughout the right atrium. The area
was consistent with the site of earliest activation
visualized in electrograms at 24 ms prior to P-wave
onset (Figure 3B).
Low-amplitude, discrete
potentials were recorded at that site. Entrainment
pacing showed perfectly concealed entrainment
(post-pacing interval minus tachycardia cycle
length of <10 ms). Therefore, this area was revealed
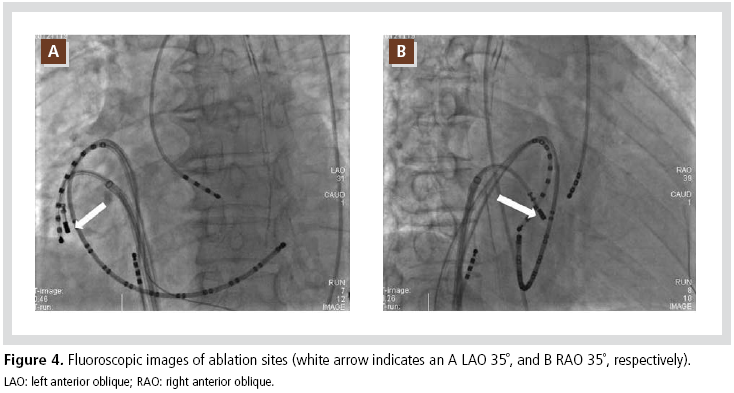
as the critical tachycardia focus. Focal ablation at
the site of earliest signal with an open irrigated tip
catheter immediately terminated the tachycardia,
which was thereafter non-inducible. Fluoroscopic
and 3-dimensional images of the ablation sites are
shown in Figures 4 and 5, respectively.
The induction test was repeated and no AT or AF was
inducible. The patient was successfully discharged
without procedure-related complications and she
has remained free of symptomatic recurrence of
arrhythmia for 2 months.
Discussion
The present case shows that a single area of slow
conduction at the crista terminalis may act as the
critical tachycardia isthmus for atypical AT. This
case further emphasizes the advantages of a 3-
dimensional voltage and activation map to identify
the mechanism of the tachycardia and slowconducting
isthmuses at uncommon sites. The
slow-conduction area on the activation map was
proved to be the critical isthmus by arrhythmia
termination during ablation.
Radiofrequency catheter ablation is the treatment
of choice for several cardiac arrhythmias. The
conventional approach using intracardiac electrograms
during sinus rhythm or tachycardia has
inherent limitations. Localization and demonstration
of the focus or entire reentrant circuit with
conventional mapping catheters remains difficult.
Furthermore, conventional mapping techniques
(i.e., pacing maneuvers) are limited by the risk of
tachycardia termination or conversion to a
nonclinical arrhythmia.1 Moreover, 2-dimensional
fluoroscopic imaging limits the ability to evaluate
several potential sites for ablation and to go
precisely to the most suitable site. Recently, 3-
dimensional mapping became popular during
electrophysiologic investigations and catheter
ablation. The mechanism of tachycardia can be
easily determined, and the wave front propagation
and the scar zone that contributes to the
tachycardia can be documented. Therefore, the use
of a 3-dimensional mapping system may improve
procedural outcomes and clinical success.2 In
particular, the efficacies of 3-dimensional mapping
of atypical atrial flutter or AT following cardiac
surgery were reported.3,4 The accurate identification
of tachycardia isthmus by creating a voltage and
propagation map and then minimizing the ablation
lesion may also avoid late recurrence of scarrelated
atypical flutter or AT.
In conclusion, 3D mapping may be particularly
helpful in patients who have recurrent atrial flutter
or AT following a previous ablation because it can
identify the slow-conduction zone or breakthrough
site and the scar zone easily-which can then be
precisely targeted.















 The induction test was repeated and no AT or AF was
inducible. The patient was successfully discharged
without procedure-related complications and she
has remained free of symptomatic recurrence of
arrhythmia for 2 months.
The induction test was repeated and no AT or AF was
inducible. The patient was successfully discharged
without procedure-related complications and she
has remained free of symptomatic recurrence of
arrhythmia for 2 months.

