International Journal of Arrhythmia 2013;14(4): 26-33.
Untitled Document
ECG & EP CASES
Ablation of Ventricular Tachycardias With Left Ventricular Apical Endocardial and Epicardial Exit Sites in a Patient With Nonischemic Cardiomyopathy
Man-Young Lee, MD, PhD Cardiology Division, Department of Internal Medicine, St. Mary’s Hospital, Catholic University of Korea
Introduction
Sustained monomorphic ventricular tachycardia (VT) with structural heart disease is often associated
with areas of ventricular scarring comprised of surviving myocytes and fibrotic tissue. After myocardial
infarction (MI), scarring involving the endocardium
is typically evident, and most re-entry
circuits causing VT can be ablated from the endocardium.1
Sustained monomorphic VT also occurs in
dilated cardiomyopathies (DCM) that are not associated
with coronary artery disease, although at a
lower frequency. Re-entry within the myocardium
is the most common cause, although bundle branch
re-entry and focal VT also occur.2-5 Catheter ablation
for VT due to myocardial re-entry in DCM is
generally thought to be more difficult than ablation
in patients with previous myocardial infarction. In
some cardiomyopathies, such as Chagas disease, the
presence of epicardial re-entry circuits that cannot
be ablated with an endocardial approach contributes
to this difficulty.6
Recently, a method of plotting low-amplitude
regions of scarring on 3-dimensional anatomic reconstructions
of the ventricle has been successfully
used to mark infarct regions and dense unexcitable
scarring that serves as a conduction block in these
regions causing VT.7,8 The locations of low-amplitude
bipolar electrograms (EGM) correlate well with
the location of the infarct scars in animal models.9 In
this report, we demonstrate the relationship between
monomorphic VTs and areas of low-amplitude
scarring through 3-dimensional electroanatomic
ventricular mapping of the endocardium, and VTs to
have 2 different exits, one from the endocardium and
another from the epicardium.
Case Report
A 76-year-old woman with a history of CHF, who
has been treated at our institution from March 2009,
received a dual chamber implantable cardioverterdefibrillator defibrillator
(ICD) because her left ventricular (LV) ejection fraction was 34% with fast inducible VTs.
At the start of the year 2013, the patient complained
of worsening palpitations, which resulted
in frequent anti-tachycardia pacing (ATP) and ICD
shocks. These episodes became more frequent, and
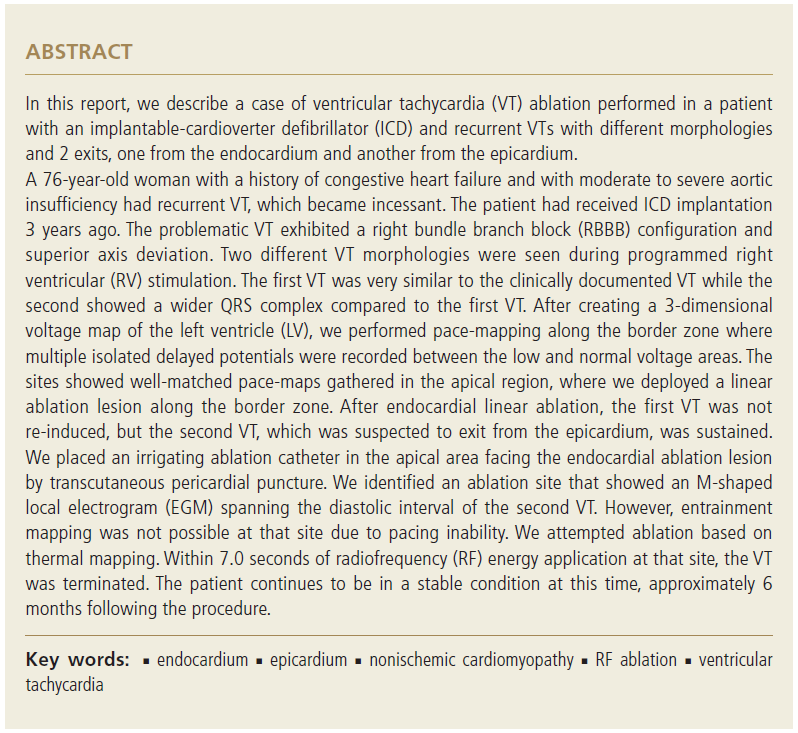
her 12-lead electrocardiogram (ECG) documented
a sustained monomorphic VT that exhibited a
right bundle branch block (RBBB) configuration and
superior-axis deviation (Figure 1). A 12-lead ECG
during sinus rhythm revealed a left axis deviation,
indicating a left anterior hemiblock.
In May 2013, a radiofrequency (RF) catheter ablation
procedure was planned as her VT became incessant
despite the use of medications including amiodarone,
which she continued to take up until the
procedure.
Electrode catheters were positioned in the high
right atrium (HRA), right His bundle (HIS), and right
ventricular apex (RVA). At baseline, the patient exhibited
normal AH (75 ms) and HV (35 ms) intervals
with a sinus cycle length of 934 ms. The clinical
VT was easily induced by pacing from the RVA. The
VT was entrained from the RV pacing and exhibited
constant fusion. Two different forms of VTs were
induced (Figure 2). Both VTs were noted to have
a similar RBBB pattern and axis. The first VT was
morphologically similar to the clinically documented
VT. The second VT was faster and wider in the
duration of QRS. The LV was mapped by a 4-mm
tip ablation catheter, which was deployed through
the left atrium by transeptal atrial puncture using
a Mullin sheath, and a 3-dimensional voltage map
of the LV was created. A well-matched pace-map
with a stimulus-QRS interval of 20 ms was obtained
at the LV interior wall near the apex, implying that
the exit site of the first VT was located nearby. After
creating a 3-dimensional map of the LV, the clinical VT was not reproducibly induced and RF catheter
ablation was performed along the border zone
at the LV apical region (Figure 3). After linear ablation
of the endocardial aspect, the first VT could
not be re-induced. However, the second VT was still
re-inducible. The wider QRS duration of the second
VT led us to speculate that it was coming from the
epicardium.
We performed transcutaneous pericardial puncture to place the ablation catheter in the pericardial
space (Figure 4). During epicardial mapping near the
bottom of the LV apex, roughly facing the area of the
endocardial linear lesion, we were able to identify a
site that showed an unusual M-shaped local EGM.
The local EGM resembled a far-field potential because
of the lack of high frequency potential, but the
duration of local EGM seemed to span the diastolic
interval of the VT. Because pacing was not possible from the epicardial mapping catheter, we decided to
attempt thermal mapping. Within 7.0 seconds of RF
energy application at that site, the VT was terminated
(Figure 5). We delivered RF energy at that site
for 60 seconds. Following this, there were no more
inducible VTs. The patient continues to remain stable
at this time, 6 months after the ablation procedure.
Discussion
This case defines the substrate causing VT in patients
with DCM and supports myocardial fibrosis
as an important factor. As acknowledged above,
myocardial re-entry was the most common cause
of sustained VT.2 In this case, the re-entry circuits
were closely related to regions of low-amplitude
EGMs, consistent with scarring, and in agreement with the findings of previous studies.4, 10
In studies of explanted hearts, de Bakker et al.11
found unexcitable fibrosis creating regions of conduction
block and surviving myocardium creating
potential re-entry circuit paths after infarction and
in DCM. Slow conduction through muscle bundles separated by interstitial fibrosis can create a zig-zag
path, producing slow conduction that promotes reentry.
The cause of fibrosis in cardiomyopathy (CMP) is not well defined. Scattered regions of replacement
fibrosis are commonly seen at autopsy, but confluent
regions of scarring are not common.11, 12
Sustained monomorphic VTs in DCM are usually caused by re-entry associated with low-voltage
areas consistent with scarring. In the patients with
nonischemic CMP, the scar areas involved in the
reentrant VT path are often known to be adjacent to
a valve annulus; they extend deep into the endocardium,
and can be transmural or greater in extent on
the epicardium than on the endocardium.
Although the arrhythmic substrate in patients with
myocardial re-entry VT in DCM has several similarities
to that in patients with previous infarction, low
voltage areas of scarring observed in DCM were
frequently adjacent to a valve annulus, as is often
the case in VT after inferior wall infarction.13, 14
The annulus sometimes seems to form a border
for an isthmus in the re-entry path.
It is interesting to speculate that the formation
of a long channel, or isthmus, along an annulus
contributes to the formation of re-entry circuits
that can support sustained monomorphic VT.
Pacing demonstrated slow conduction in these regions
with long S-QRS delays during pace mapping
and entrainment. However, in this present
patient who had no history of MI, the echocardiogram
interestingly showed apical aneurysm
formation which was not noted at the time of ICD
implantation, indicating the plausible interrelation
between ICD lead placement in the RV apex
and the worsening of apical wall motion. Even
though the mechanism of apical aneurysm formation
in this patient was uncertain, the mapping
study showed that the VT exit site was adjacent to
the apical region.
The success rate of endocardial ablation for
nonischemic CMP was lower than that of postinfarct
VT2. Re-entry circuits deep in the endocardium
and in the epicardium appear to be
a likely explanation. Epicardial mapping led to
successful ablation in more than half of the patients in whom it was attempted. The successful
ablation sites were again associated with lowamplitude
regions. Pacing in these regions also
showed evidence of slow conduction. Interestingly,
the region of low amplitude was strikingly
larger in the epicardium than at the endocardium.
The importance of epicardial re-entry circuits in
CMP was demonstrated by Sosa et al.6 for patients
with Chagas disease, in whom approximately 70%
of VTs were epicardial in origin. Recently, Hsia
et al.10 used limited epicardial mapping via the
coronary venous system to demonstrate epicardial
involvement in the re-entry circuits in 3 of 19
patients with CMP unrelated to Chagas disease.
In terms of ECG criteria for prediction of an epicardial
origin of VTs, several ECG markers need
to be emphasized. Activation from an epicardial
origin produces a widening of the initial part of
the QRS complex, visible on a conventional surface
ECG as a pseudo delta wave. The presence
of a Q wave in the limb leads also suggests an
epicardial origin of VTs. The wide QRS duration of
VT could be a marker of epicardial origin as well.
The wider QRS of the second VT compared to the
first VT led us to speculate on the possibility of an
epicardial origin of VT in this patient, which was
confirmed by the epicardial abolition of the VT.
Although safe epicardial ablation has been reported
by others,6, 15 in this present case, about
600 mL of blood drained through the pericardial
sheath for a day. Fortunately, the bleeding
stopped spontaneously. Prudent precautions must
be taken to avoid coronary artery and phrenic
nerve injury. We performed coronary angiography
while the ablation catheter was on a target site to
assess the distance to the coronary artery and also
attempted epicardial pacing to detect proximity to
the left phrenic nerve, which, however, was not possible.
Because it is desirable to achieve pericardial
access before systemic anticoagulation for endocardial
LV mapping, performing epicardial mapping
before LV endocardial mapping in DCM is a
reasonable consideration. This approach must be
balanced, however, by anticipated risks and the
experience of the team with the epicardial approach,
because many VTs can be ablated from
the endocardium.
Conclusions
The patient described in this case report, however,
exhibited a VT originating from the apical region,
which showed aneurysmal change, indicating a possible
connection to ICD lead placement. Combined
endocardial and epicardial mapping approaches are
likely to improve the success of ablation.