동성 빈맥
Sinus Tachyarrhythmia
Article information
Trans Abstract
Sinus tachycardia is an accelerated rhythm in which the rate of impulses arising from the sinoatrial node is elevated. Uncontrolled sinus tachycardia may result in a poor prognosis, particularly in patients with cardiovascular disease, because of a hemodynamic disturbance arising from the tachycardia itself. When sinus tachycardia is specifically triggered by anemia, shock, or fever, it is referred to as physiological sinus tachycardia. Physiological sinus tachycardia should resolve with correction of the underlying cause. Inappropriate sinus tachycardia (IST) is unexplained by physiological demand. Palpitation is the most frequent symptom in IST patients. Even though treatment of IST has insufficient efficacy and a relatively high recurrence rate, several treatment strategies such as use of a β-blocker, ivabradine, and radiofrequency catheter ablation can be used for IST patients.
서론
안정 시의 심박동수는 주로 미주신경 긴장도에 영향을 받아 결정되며 [1–4], 연령에 따른 정상 심박동수의 분포가 다르기는 하나 보편적으로 분당 맥박수가 100회 이상일 경우를 빈맥, 60회에서 100회 미만까지를 정상 범위로 정의하고 있다. 동성 빈맥은 동방결절(sinoatrial node)에서 시작한 박동의 빈도가 증가되어 발생하며, 임상에서 흔하게 접하면서도 쉽게 중요성이 간과되기도 하는 부정맥이다. 실제로 기저 심장 질환이 있는 환자는 심장 질환의 악화 이외의 원인에 의한 동성 빈맥이라고 하더라도 방치할 경우 예후가 악화될 수 있다 [5,6]. 심전도 상 동방결절에서 기인하는 형태의 P파는 사지유도인 I, II, aVF에서 양성파로 나타나며, 전 흉부 유도인 V1에서 이상성(biphasic)으로 나타난다. 동방결절 회귀 빈맥이나 동방결절에 인접한 부위에서 기인하는 심방빈맥에서도 유사한 모양의 P파가 보일 수 있으며, 이는 심장 전기생리학 검사를 통해서 감별이 가능하다. 이번 리뷰에서는 생리적 현상으로 발생하는 동성 빈맥과 특이 유발 요인이 없는 상태에서 발생하는 부적합 동성 빈맥(inappropriate sinus tachycardia, IST)의 원인과 양상 및 치료에 대해서 검토해 보려고 한다.
생리적 동성 빈맥
생리적 동성 빈맥(physiological sinus tachycardia)은 저혈량성 쇼크, 빈혈, 심부전, 갑상선항진증 등 병적인 상태나 교감신경계를 항진시키거나 미주신경을 억제하는 약물, 마약 등에 노출되는 경우, 통증이나 심리적 긴장 상태 등에서 발생할 수 있으나(Table 1), 기저 원인 질환 등의 상태를 호전시키면 회복될 수 있다.
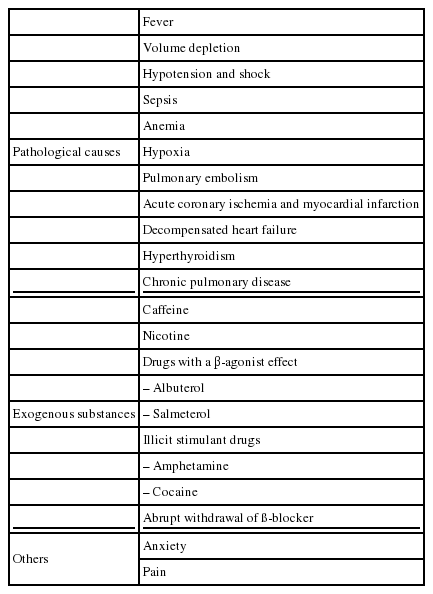
Causes of physiological sinus tachycardia
일반적으로 생리적 동성 빈맥 자체로는 증상이 없는 경우가 많으나, 빈맥으로 인한 혈역학적 변화로서 좌심실 충만 시간 감소에 따른 심박출량 감소, 심근의 산소 요구량 증가, 관상동맥 혈류량 감소 등이 발생하므로 특히 기저 심장 질환 환자에게 호흡곤란이나, 흉통 등의 증상이 유발되거나 예후를 악화시킬 수 있다. 따라서 빈맥 유발 요인에 대한 정확한 병력 청취와 발열, 빈혈이나 저혈량 등을 평가하는 이학적 검사의 중요성을 간과하지 말아야 한다.
유발 요인에 대한 조사 이외에도 24시간 심전도 모니터링 등을 시행하여 맥박수의 변화가 점진적이지 않고 급격한 변화를 보이는지 또는 안정 시 및 수면 중의 빈맥 여부를 확인함으로써 발작성으로 나타나는 방실결절 회귀 빈맥이나 심방빈맥, IST 등과의 감별에도 도움을 받을 수 있다.
부적합 동성 빈맥(IST)
IST란 생리적, 병리적 또는 약물 등에 의한 기전으로 설명되지 않는 동성 빈맥으로 정의되며, 안정 시의 분당 심박동수가 100회 이상이거나, 24시간 Holter 모니터링 상의 평균 심박동수가 90회 이상인 경우를 말한다 [2]. 대개의 환자들에서 심계항진이나 전실신 같은 증상이 나타나며, 젊은 여성에서 호발한다 [7,8]. 발생 원인에 대한 병태생리학적 기전은 구체적으로 밝혀지지는 않았으나, 자율신경기능장애, 신경호르몬(neurohormone) 이상, 동방결절의 내인성 과다활동(intrinsic sinus node hyperactivity) 등에 기인하는 것으로 알려져 있다 [2].
IST의 진단은 감별해야 할 다른 빈맥을 배제한 후에야 이루어질 수 있으며, 감별해야 할 부정맥으로는 생리적 동성 빈맥, 동방결절 인근에서 기인하는 심방빈맥, 자세 변화에 따른 기립성 빈맥 증후군(postural orthostatic tachycardia syndrome, POTS) 등이 있다 [8]. POTS는 기립 시에 혈압의 저하 없이 심박동수가 현저히 증가하는 상태를 말하며, 정상 심장을 가진 젊은 여성에서 호발하고, 동방결절의 맥박수를 낮추는 약제를 사용하면 심한 기립성 저혈압이 유발될 수 있기 때문에 감별진단에 주의해야 한다.
부적합 동성 빈맥의 치료
IST의 예후는 일반적으로 양호하기 때문에 치료는 증상을 감소시키는 데 초점을 두고 이루어지며, 경우에 따라서는 치료를 고려하지 않기도 한다. 안타깝게도 IST의 치료는 어려운 편이며, 심박동수의 감소가 증상의 호전으로 이어지지 않는 경우도 많다.
베타차단제나 칼슘차단제를 통해서 심박동수를 감소시키는 치료는 그다지 효과적이지 못하며, 저혈압 등의 부작용으로 인해 순응도가 떨어지는 경우가 많고, 운동요법으로 효과를 기대할 수도 있다는 보고가 있으나 입증되지는 않았다.
Ivabradine은 I-funney (I f) 채널을 길항하여 동방결절의 자동능을 감소시키는 약물로서 동방결절의 박동조절기(pacemaker) 활동성을 억제하여 다른 혈역학적 효과에 대한 영향 없이 심박동수만을 감소시키는 약제이다. 분당 심박동수가 70회 이상이면서 좌심실 박출률이 35% 이하인 심부전 환자에게 효과가 입증되어 사용이 허가된 상태이며, 정식으로 승인되지는 않았으나 약제의 기전에 근거하여 여러 보고에서 IST의 치료에도 적용하며, 효과를 보여주었다 [9–14]. Ptaszynski P 등은 IST의 치료제로 metoprolol과 ivabradine 을 비교하였는데, 두 가지 약제에서 심박동수의 감소 효과는 유사하였으나 증상은 ivabradine군에서 더 크게 감소하는 경향을 보여 주었으며 [14], Cappato R 등은 ivabradine과 위약의 비교 연구에서 ivabradine의 증상 개선 효과와 운동 능력 향상 효과를 보여주었다 [10]. 이러한 연구 결과를 토대로 2015년 미국부정맥학회에서는 IST의 증상 개선을 위한 치료제로 ivabradine의 사용을 긍정적으로 언급하고 있다 [7,8]. Ivabradine의 부작용으로 심방세동의 발생이 증가할 수 있는데, 심방세동의 발생 시에는 약제의 중단이 권고된다.
또 다른 치료법으로 고주파전극도자절제술(radiofrequency catheter ablation, RFCA)을 이용하여 동방결절을 변형(modification)시킴으로써 심박동수를 감소시키는 방법이 있으며, 코호트 연구에서 초기 성공률은 76–100%로 보고되고 있다 [15–18]. 하지만 수개월내 IST의 재발률이 27%로 보고되며, IST의 재발 없이 증상만 재발되는 경우까지 합하면 45%의 재발률이 보고되고 있기 때문에 RFCA 시에 발생할 수 있는 합병증의 심각성을 고려하면 약물 치료에 반응하지 않고 증상이 매우 심한 IST 환자에게만 위험성에 대한 충분한 사전 설명과 함께 선택적으로 시행하는 것이 권고된다.
결론
동성 빈맥은 임상에서 흔하게 접하는 빈맥이다. 대부분은 자율신경계에 영향을 미치는 특정 유발 요인이 선행하여 발생되는 생리적 동성 빈맥이며, 빈맥에 의한 혈역학적 변화가 기저 심장 질환 환자에게 증상 악화를 초래할 수 있음을 인지하고, 기저 유발 요인의 교정을 시도해야 한다. IST의 경우는 드물게 접하게 되고, 비교적 예후가 좋은 편이며, 환자의 증상을 개선하기 위해서 약물 치료를 시작으로 고주파전극도자절제술까지 치료법의 단계적인 적용이 가능하다.
References
Biography
Gu-Hyun Kang, MD
