|
|
International Journal of Arrhythmia 2011;12(2): 39-40.
|
Case
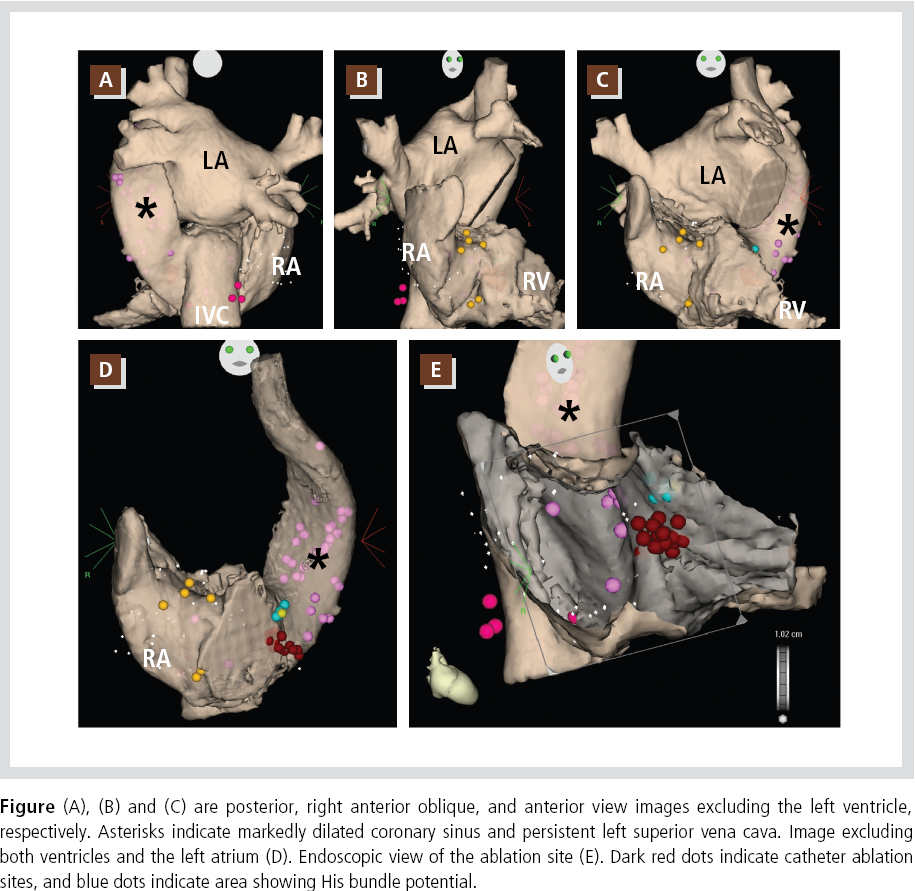
A 65-year-old man was re-evaluated for recurrent narrow QRS tachycardia. Twelve months
ago, a cardiac electrophysiological study (EPS) failed to induce tachycardia, but revealed absent
right and persistent left superior vena cava (SVC).
A cardiac CT scan was obtained for image integration before EPS. The electroanatomical
mapping system was used with CartoMerge
software (Biosense-Webster, Diamond Bar, CA).
The figure shows 3D images reconstructed by
image integration software. The reconstructed
images clearly prove the absence of right SVC as
well as persistent left SVC with markedly dilated
coronary sinus (Figure, A-D). Atrioventricular
nodal reentrant tachycardia (AVNRT, slow/fast
type) was reproducibly induced by programmed
electrical stimulation. Catheter ablation was
successfully performed at the rim of the coronary
sinus ostium just below the His-bundle potential
area (Figure, E). After ablation, tachycardia was
not inducible.
Discussion
Persistent left SVC alone is not uncommon, but a
case with absent right and persistent left SVC is a
rare congenital anomaly. Koch’s triangle, which is
surrounded by the tendon of Todaro and the
coronary sinus ostium, is a critical structure in
catheter ablation for AVNRT. However, the
anatomical structure of this area is severely
deformed in this congenital anomaly due to a
markedly dilated coronary sinus. Therefore, the
anatomical information is important and the
ablation procedure is challenging. In the previous
reports, successful ablation sites were not usually
slow-pathway areas but the rim of the coronary
sinus ostium near the atrioventricular node as the
present case.1,2 A 3D mapping system can give us
more precise anatomical information to help to
target the appropriate site. In the present report,
we demonstrate usefulness of an electroanatomical
mapping system, and provide images with rich
anatomical information. A catheter navigation
system may facilitate the procedure as well.3
References
- 1. Okishige K, Fisher JD, Goseki Y, Azegami K, Satoh T, Ohira H,
Yamashita K, Satake S. Radiofrequency catheter ablation for av
nodal reentrant tachycardia associated with persistent left
superior vena cava. Pacing Clin Electrophysiol. 1997;20:2213-
2218.
- 2. Pitzalis MV, Forleo C, Luzzi G, Anaclerio M, Barletta A, Di Biase M, Rizzon P. Successful ablation of atrioventricular nodal reentry
tachycardia in a patient with persistent left superior vena cava.
Cardiologia. 1998;43:741-743.
- 3. Ernst S, Ouyang F, Linder C, Hertting K, Stahl F, Chun J, Hachiya
H, Krumsdorf U, Antz M, Kuck KH. Modulation of the slow
pathway in the presence of a persistent left superior caval vein
using the novel magnetic navigation system niobe. Europace.
2004;6:10-14.
|
|
|
|












