International Journal of Arrhythmia 2012;13(4): 29-33.
Untitled Document
ECG & EP CASES
A Case of Cerebral Infarction in Atrial Fibrillation Caused by Interruption of Warfarin Therapy for Colonoscopy
한림대학교 의과대학 내과학교실 한 상 진
Sang-Jin, Han, MD Cardiology Division, Department of Internal Medicine, Hallym University College of Medicine, Anyang, Korea
Introduction
Warfarin is widely used in cases of atrial fibrillation (AF), venous thromboembolism (VTE),
mechanical heart valve use, and stroke. Endoscopic procedures (e.g., esophagogastroduodenoscopy
[EGD], colonoscopy, and sigmoidoscopy) are often used in Korea.
For AF with a high thromboembolic risk, bridging anticoagulation is used before such procedures.
Because bridging therapy is expensive and time consuming, the procedure is instead performed
with interruption of warfarin therapy in many
cases.
We report a case wherein a patient with atrial fibrillation experienced a stroke when he
temporarily stopped warfarin treatment in preparation for a colonoscopy.
Case
A 75-year-old man was admitted to the emergency room (ER) for dysarthria that was
observed 4 hours earlier. When he arrived, body temperature was 36.0°C, pulse rate was 84 beats
per minute with irregular beats, and blood pressure was 170/90 mmHg.
On neurologic examination, pupillary light reflex was prompt and he displayed isocoria. His eyes had
a right-side deviation, visual field showed left hemianopsia, left facial motor tone had decreased,
and peripheral motor tone was intact. His initial NIH stroke scale rating was 8 and his Glasgow coma scale score was 11.
Laboratory studies showed that the patient's prothrombin time (PT) was 15.2 s (normal range
11.5~14.0 s), and PT international normalized ratio (INR) was 1.20, activated partial thromboplastin
time (aPTT) was 30.6 s (normal range, 28.0~41.0 s);
a random plasma glucose test showed that the
plasma glucose level was 300 mg/dL (normal 70~110 mg/dL). The results of other laboratory
tests were within normal limits.
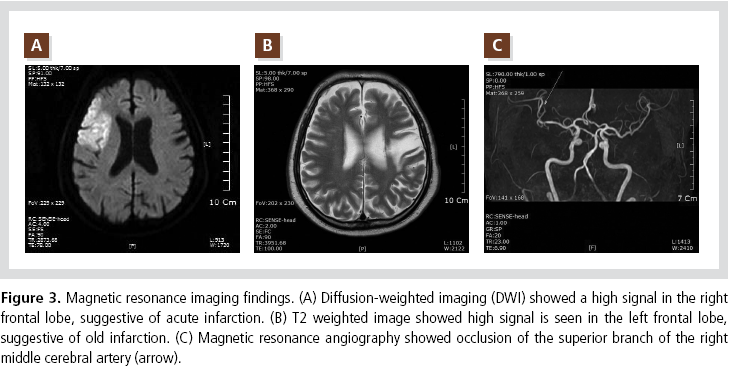
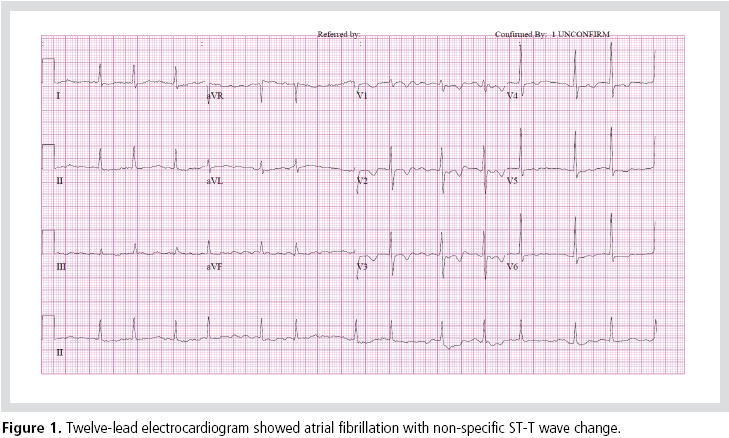
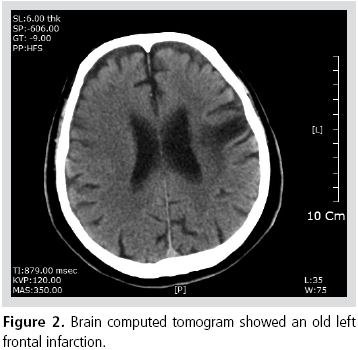
Atrial fibrillation was detected in the ER (Figure 1). A computed tomogram (CT) (Figure 2) showed an
old infarction in the left frontal lobe, but no sign of
hemorrhage. Subsequent magnetic resonance imaging (MRI) (Figure 3 A, B, and C) identified an
acute infarction in the right frontal lobe. However,
because the symptom had occurred more than 3 hours earlier, thrombolysis was not performed.
The patient was under medical treatment because
of a left middle cerebral artery (MCA) infarction
that had developed 14 years earlier, as well as for hypertension and diabetes mellitus. He had been
taking warfarin as an outpatient and had a CHADS2
score of 5.
Interruption of warfarin therapy for colonoscopy had been recommended to the patient and the event
occurred 3 days after this interruption of therapy.
His symptoms improved after conservative management and he was subsequently discharged.
Discussion
Many patients receive long-term treatment with
warfarin because of AF, a mechanical heart valve,
or VTE. Such patients frequently require warfarin
therapy to be interrupted because of an upcoming
surgery, tooth extraction, or invasive procedure.
The current European and US cardiology AF
guideline1 recommends that bridging treatment
should not be used in low-risk cases, but does
recommend bridging in cases where the patient has a
mechanical valve, a high risk of thromboembolism,
or the therapy would need to be interrupted for
more than 7 days.
It is uncertain whether such patients should
receive bridging anticoagulation before and after a surgery or procedure. One study2 provided data on
warfarin interruption in 492 patients (43% had AF)
for surgery or a procedure. Bridging therapy was
not used for 54% of the patients, while bridging
with a therapeutic dose of heparin products was
used for 33% of patients. Major bleeding occurred
significantly less often when bridging therapy was
not used (1.1%) than when bridging with a
therapeutic dose of heparin products was used
(6.8%); the difference was statistically significant.
Thromboembolism occurred in 1.1% of cases where
bridging therapy was not used and in 0% of cases
where such bridging therapy was used; however,
the numbers were too small for statistical
comparison. The risk of major bleeding is strongly
associated with the use of postoperative therapeutic
doses of heparin products.
Another study3 was performed on 1,024 patients
who underwent 1,293 interruptions of warfarin
therapy for surgery or a procedure. Fifty-four
percent of the patients had AF and 8.3% of the
patients underwent bridging therapy with heparin
products. The most common procedures were
colonoscopy (25%) and oral or dental surgery (25%).
More than 80% of patients underwent interruption of warfarin therapy for 5 days or less. After 30 days
of interruption, thromboembolism occurred in 0% of
the patients who underwent bridging therapy and
in 0.6% of patients who did not. Major bleeding
occurred in 3.7% of the patients in the former
category and in 0.2% of the patients in the latter.
A brief (≤5 days) periprocedural interruption
of warfarin is associated with a low risk of
thromboembolism. The risk of major bleeding
should be weighed against the thromboembolic risk
for an individual patient before the administration
of bridging therapy.
Because of thromboembolic risk and bleeding
risk, the interruption of warfarin and the use of
bridging therapy should be decided on a case-bycase
basis. A randomized controlled trial (RCT),
termed the BRIDGE study (bridging anticoagulation in patients who require temporary interruption of
warfarin therapy for an elective invasive procedure
or surgery), are being performed.
The BRIDGE study investigators4 recommend the
use of bridging anticoagulation therapy according
to thromboembolic risk (Table 1). The 2010
Canadian guidelines5 recommend that low bleeding
risk for a surgery or procedure should not require
interruption of warfarin therapy or consideration of
bridging therapy. The 2009 American Society for
Gastrointestinal Endoscopy (ASGE) guideline6
recommends not interrupting warfarin therapy for
diagnostic tests (EGD, colonoscopy, or flexible
sigmoidoscopy) including biopsy, as they are lowrisk
procedures.
However, these guidelines are not followed
robustly in clinical situations. In a survey7 of patients who temporarily stopped warfarin therapy,
it was found that 57% had AF and 50% of the
respondents had received at least 1 request for a
periprocedural interruption of warfarin therapy
during the prior 12 months. Nearly half (48%) of all
requests to interrupt warfarin therapy were for
guideline-discordant indications.
Because we expect a higher ratio in Korea,
educational interventions may decrease the risk of
periprocedural thromboembolic complications.
References
Fuster V, Ryden LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen
KA, Halperin JL, Heuzey JYL, Kay GN, Lowe JE, Olsson SB,
Prystowsky EN, Tamargo JL, Wann S, Smith Jr. SC, Jacobs AK,
Adams CD, Anderson JL, Antman EM, Halperin JL, Hunt SA,
Nishimura R, Ornato JP, Page RL, Riegel B, Priori SG, Blanc AB,
Budaj A, Camm AJ, Dean V, Deckers JW, Despres C, Dickstein K,
Lekakis J, McGregor K, Metra M, Morais J, Osterspey A, Tamargo
JL, and Zamorano JL. ACC/AHA/ESC 2006 Guidelines for the
Management of Patients With Atrial Fibrillation: A Report of the
American College of Cardiology/American Heart Association Task
Force on Practice Guidelines and the European Society of
Cardiology Committee for Practice Guidelines (Writing
Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation): Developed in Collaboration With
the European Heart Rhythm Association and the Heart Rhythm
Society.
Circulation.
2006;114:e257-e354.
The BRIDGE study investigators. Bridging anticoagulation. Is it
needed when warfarin is interrupted around the time of a surgery
or procedure?
Circulation.
2012;125:e496-e498.











 On neurologic examination, pupillary light reflex was prompt and he displayed isocoria. His eyes had
a right-side deviation, visual field showed left hemianopsia, left facial motor tone had decreased,
and peripheral motor tone was intact. His initial NIH stroke scale rating was 8 and his Glasgow coma scale score was 11.
On neurologic examination, pupillary light reflex was prompt and he displayed isocoria. His eyes had
a right-side deviation, visual field showed left hemianopsia, left facial motor tone had decreased,
and peripheral motor tone was intact. His initial NIH stroke scale rating was 8 and his Glasgow coma scale score was 11.